
“Trulicity was heavily marketed to doctors despite a high NNT, number needed to treat. NNT tells you how many patients need to be treated and for how long for one patient to benefit from the drug. It turns out that we have to treat 327 people for three years to prevent one non-fatal heart event, and that treatment costs $2.7 million.”
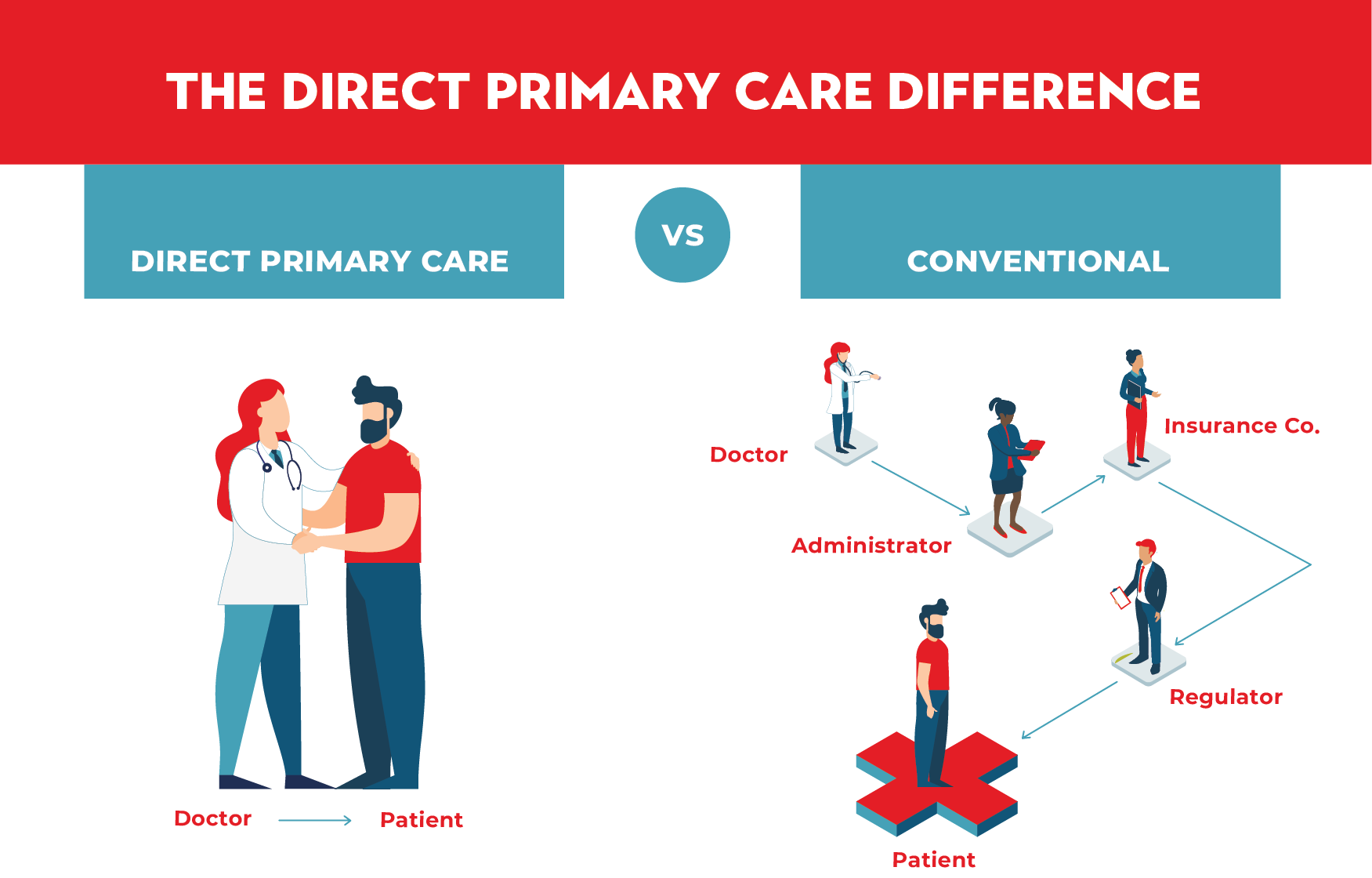
“I happened to mention this to a DPC friend and she said, “We don’t even prescribe that.” Wow! There’s an advertisement for the value of DPC if I ever heard one! DPC doctors’ interests are aligned with those of their patients. They don’t prescribe expensive meds with questionable efficacy.”
By Gayle Brekke
I love spring because it’s new life! Yes, more of my plants are coming to life, but so are the weeds. Oh well. Being outside in the sunshine pulling weeds gives me time to think about fixing health care and how blessed I am that you are here with me. I’m thrilled with all of the new people who’ve connected with me and who are reading this newsletter and listening to the podcast. I appreciate you!
This is Gayle Brekke with Primary Care Mindset. On the next episode of my Nurturing the Heart of Family Practice podcast, I’ll tell you more about me and why I’m so enamored with Direct Primary Care. Today’s newsletter is to let you know I’m excited about ramping up engagement with you soon, and to give you a sneak peek of what to look forward to.
I will soon be hitting the gas on the podcast and newsletter because I’m finally “SDC” regarding my PhD – SO DARN CLOSE!
Great ideas for health care improvement are out there but you likely need help seeing them. Maybe you wonder what we can do differently because we’ve been trying to fix health care for decades. Maybe you feel helpless in the face of enormous health care challenges. That’s where I come in. My outsider perspective and questioner nature will open your eyes to solutions you had not considered. I promise. Here’s why I think differently.
I Look at Things Differently.
I initially dove into health care many years ago because its terrible results despite huge efforts of throngs of different professionals intrigued me. I was quickly convinced that such results could only happen if there were serious long-standing problems with our thinking at a fundamental level.
As an outsider to medicine (I have no clinical training) but not to the financing of health care and health insurance (I’m a health actuary and health services researcher), my training may differ from yours, although lots of actuaries are newsletter subscribers. (Hi guys!) Add to that my secret power of questioning and that’s why my unique way of looking at health care offers dramatically better results.
I am a Questioner.
When I’m intrigued by something, I keep asking questions until it makes sense to me. In her book, The Four Tendencies, Gretchen Rubin delineates four types of people based on whether they meet or resist internal and external expectations. Questioners resist outer expectations and meet inner expectations. We comply with external expectations if they make sense to us.
The Trulicity story below illustrates how I think differently about health care challenges and solutions. This is an example of what you can expect in future newsletters and podcast episodes.
A Sneak Peak of What’s Coming Up – Trulicity.
I recently came across the text from a speech by John Abramson, physician and author of Sickening: How Big Pharma Broke American Health Care and How We Can Repair It. He said that Trulicity was heavily marketed to doctors despite a high NNT, number needed to treat. NNT tells you how many patients need to be treated and for how long for one patient to benefit from the drug. It turns out that we have to treat 327 people for three years to prevent one non-fatal heart event, and that treatment costs $2.7 million! Obviously, this is a huge problem. (My point isn’t about one particular drug; this is just an illustrative example.)
Dr. Abramson’s prescription for this problem involved top-down changes including how research is funded, how academic journals review and publish research, and how we as a country evaluate the value of innovations and negotiate prices.
I have an entirely different take, which revolves around a story of a patient ahead of me in line at the pharmacy. An elderly man was picking up Trulicity. His coverage had changed and his cost was a whopping $1,200. He said that he’d have to go home and get a different credit card because he needed the medicine. My heart went out to him and I was thinking that he would have simply called his doctor’s office if he had DPC, to verify that he needed the medicine and there wasn’t anything less expensive he could take instead.
I happened to mention this to a DPC friend and she said, “We don’t even prescribe that.” Wow! There’s an advertisement for the value of DPC if I ever heard one! DPC doctors’ interests are aligned with those of their patients. They don’t prescribe expensive meds with questionable efficacy.
Thinking Differently: DPC is a Bottom-Up Solution that Anyone can Deploy
It is my belief that bottom-up solutions are usually superior to top-down solutions. For one thing, bottom-up solutions are available to essentially everyone. We all have more power to affect our situation than we usually realize and DPC is a great example of how bottom-up thinking leads to dramatically better results.
I Need Your Help.
Please consider passing this newsletter along to others who may be interested. They can subscribe to my mailing list here. Also, check out my podcast, Nurturing the Heart of Family Practice, available wherever you get your podcasts.
Thank you for being here with me – I can’t wait to ramp up engagement with you over the next couple months. Now I’m heading outside – the weeds are calling.
